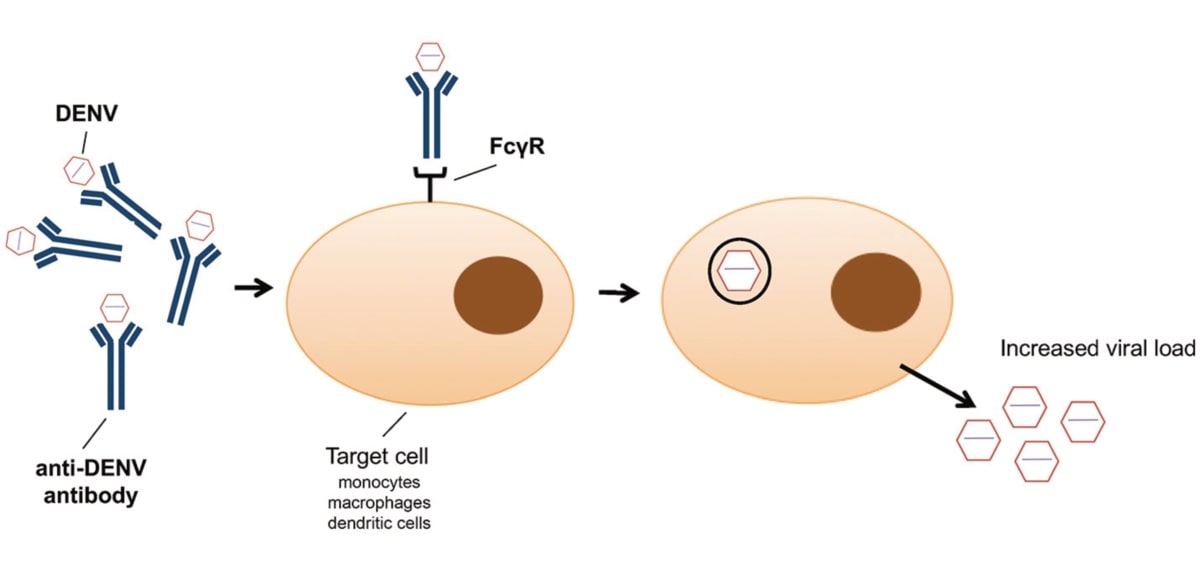
Example of antibody dependent enhancement of dengue virus1 also seen with coronavirus vaccines. Notice that the antibodies actually draw the virus into the cells, where they multiply, rather than destroying it.
A serious risk of coronavirus vaccines
A potentially fatal risk of coronavirus vaccines has been known for decades. It’s called antibody dependent enhancement (ADE). In simple terms, because of the way some viral antibodies work, they may actually backfire on the person when they subsequently encounter the wild virus. Non-neutralizing antibodies may enable the virus to enter the cells or the immune response may be skewed in other ways.
This is the reason why there has never been a coronavirus vaccine before. When they tried developing coronavirus vaccines in the past, the test animals seemed to develop robust antibodies but when they were challenged with the wild virus, they got sick and died. This stopped the vaccine development in its tracks. This adverse reaction has been also seen with Dengue Virus, Ebola Virus, HIV, and RSV vaccines well.
The clinical trials for the Covid-19 vaccines2 were much too short to do proper and complete animal testing; the quick move to human trials, and to Emergency Use Authorization (not approval) of the vaccine, means that the global population will be used as the test animals in this experiment. The FDA, referring to it euphemistically as “vaccine-enhanced disease”, stated as much in their briefing document where they acknowledged that ADE will more likely be seen over time, following authorization or even after licensure, as vaccine immunity begins to wane.
Since ADE could potentially take months to years to occur in the various populations and demographics around the world, we may have a looming global disaster yet to come. One microbiologist has referred to it as a “ticking time bomb”.
Not only is this risk being ignored but, so too, is halacha (Jewish law).3
Here are the details:
FDA did not approve any vaccine for Covid-19
When the FDA issued an emergency use authorization (EUA) for the Pfizer vaccine (all other FDA authorized Covid-19 vaccines being rolled out now will only be for EUA), they specifically noted in their briefing document, albeit at the very end (were they trying to bury the problem?), that the potential for this was yet to be seen4 (emphasis added):
Available data do not indicate a risk of vaccine-enhanced disease, and conversely suggest effectiveness against severe disease within the available follow-up period. However, risk of vaccine-enhanced disease over time, potentially associated with waning immunity, remains unknown and needs to be evaluated further in ongoing clinical trials and in observational studies that could be conducted following authorization and/or licensure.
Since the FDA only gave authorization, not approval and licensure, for the vaccine, they emphasized that the Covid-19 vaccine is investigational in nature and people must be told the known and potential benefits and risks. and be given the right to refuse the vaccine (see image to right which is a slide introduced during their issuance meeting.5)
An agreement between the Israeli government and Pfizer, the full details of which are being withheld from the public, to roll out their vaccine to the entire Israeli citizenry6 is why, according to Pfizer CEO Albert Bourla: ‘Israel has become world’s lab right now’. 7 Unfortunately, the Israeli government is pressuring its citizens to take the vaccine, rather than giving them the option to refuse as per the FDA, and as is required under the Nuremberg Code written after the Holocaust to protect human beings from any future unwanted medical experimentation.
More than just a theoretical risk
An article in the International Journal of Clinical Practice8 raised concerns about the lack of informed consent for trial participants because of ADE.9 From the section entitled: “The Risk of ADE in COVID‐19 Vaccines is Non‐Theoretical and Compelling” (emphasis added):
… The immune mechanisms of this enhancement have invariably involved antibodies, from direct antibody‐dependent enhancement, to immune complex formation by antibodies, albeit accompanied by various coordinated cellular responses, such as Th2 T‐cell skewing.2-7 Notably, both neutralising and non‐neutralising antibodies have been implicated. A recent study revealed IgG‐mediated acute lung injury in vivo in macaques infected with SARS that correlated with a vaccine‐elicited, neutralising antibody response.8 Inflammation and tissue damage in the lung in this animal model recapitulated the inflammation and tissue damage in the lungs of SARS‐infected patients who succumbed to the disease. The time course was also similar, with the worst damage occurring in delayed fashion in synchrony with ramping up of the immune response. Remarkably, neutralising antibodies controlled the virus in the animal, but then would precipitate a severe, tissue‐damaging, inflammatory response in the lung. …
Similarly, Phase 1 and 2 clinical trials of vaccine candidates have only been designed around immunogenicity as an efficacy end point and have not been designed to capture exposure of subjects to circulating virus after vaccination, which is when ADE/immunopathology is designed to occur. Thus, the absence of ADE evidence in COVID‐19 vaccine data so far does not absolve investigators from disclosing the risk of enhanced disease to vaccine trial participants, and it remains a realistic, non‐theoretical risk to the subjects.
Former Pfizer scientists worried
Alarm bells were sounded by former Pfizer scientists Dr. Michael Yeadon, the ex-Pfizer head of respiratory research, and Dr. Wolfgang Wodarg, the lung specialist and former head of the public health department. They applied to the EMA, the European Medicine Agency responsible for EU-wide drug approval, to immediately suspend all SARS CoV 2 vaccine studies in human beings. The possibility of ADE, which needed to be studied better before the vaccine was introduced to the public, was one of the serious adverse events that they described when they filed their application.10
From the application (emphasis added):
For a vaccine to work, our immune system needs to be stimulated to produce a neutralizing antibody, as opposed to a non-neutralizing antibody. A neutralizing antibody is one that can recognize and bind to some region (‘epitope’) of the virus, and that subsequently results in the virus either not entering or replicating in your cells. A non-neutralizing antibody is one that can bind to the virus, but for some reason, the antibody fails to neutralize the infectivity of the virus. In some viruses, if a person harbors a non-neutralizing antibody to the virus, a subsequent infection by the virus can cause that person to elicit a more severe reaction to the virus due to the presence of the non-neutralizing antibody. This is not true for all viruses, only particular ones. This is called Antibody Dependent Enhancement (ADE), and is a common problem with Dengue Virus, Ebola Virus, HIV, RSV, and the family of coronaviruses. In fact, this problem of ADE is a major reason why many previous vaccine trials for other coronaviruses failed. Major safety concerns were observed in animal models. If ADE occurs in an individual, their response to the virus can be worse than their response if they had never developed an antibody in the first place. …
A brief summary of their application can be found here.
There are many doctors and scientists, who have warned, and are warning about the dangers of Covid-19 vaccines. According to halacha, Shulchan Aruch (Orach Chaim, 618:4), when you have 2 doctors who say that there’s a risk of death, even if 100 doctors say there’s no risk, we listen to the 2 doctors. The Mishna Berurah explains: “ולא אזלינן בתר רב דעות בסכנת נפשות”(we do not follow the majority of opinions in a case of danger to life).
Is the vaccine a ticking time bomb?
Biochemist and molecular biologist, Dr. Doug Corrigan, believes it is.11 He explains that antibody dependent enhancement may not be seen for many years down the road:
This inherent unpredictability problem is highlighted in the following scenario: A coronavirus vaccine may not be dangerous initially. If the initial testing looks positive, mass vaccination efforts would presumably be administered to a large portion of the population. In the first year or two, it may appear that there is no real safety issue, and over time, a greater percentage of the world population will be vaccinated due to this perceived “safety”. During this interim period, the virus is busy mutating. Eventually, the antibodies that vaccinated individuals have floating around in their bloodstream are now rendered non-neutralizing because they fail to bind to the virus with the same affinity due to the structural change resulting from the mutation.
Corrigan also raises another serious issue with Covid-19 vaccines. Since they are only designed to produce antibodies against one protein on the outer shell of the virus, they will only be protective against a single portion of the entire virus. He explains (emphasis added):
In a real infection, our immune system is exposed to every nook and cranny of the entire virus, and as such, our immune system develops a panacea of antibodies that recognize different portions of the virus and, therefore, coat more of the virus and neutralize it. In addition, our immune system develops T-Cell responses to hundreds of different peptide epitopes across the virus; whereas in the vaccine the plethora of these T-Cell responses are absent. Researchers are already aware that the T-Cell response plays a cooperative role in either the development of, or absence of, the ADE response.
Based on these differences and the skewed immunological response which is inherent with vaccines, I believe that the risk of ADE is an order of magnitude greater in a vaccine-primed immune system rather than a virus-primed immune system.
Getting the infection is much, much safer than getting the vaccine.
Disturbed by the way vaccine manufacturers disregard the dangers of ADE, he quotes from an article in Nature magazine (emphasis added):
“It’s important to talk about it [ADE],” says Gregory Glenn, president of R&D at Novavax, which launched its COVID-19 vaccine trial in May. But “we can’t be overly cautious. People are dying. So we need to be aggressive here.”
And from the same article:
ADE “is a genuine concern,” says virologist Kevin Gilligan, a senior consultant with Biologics Consulting, who advises thorough safety studies. “Because if the gun is jumped, and a vaccine is widely distributed that is disease enhancing, that would be worse than actually not doing any vaccination at all.”
What would be the motivation for a vaccine manufacturer to throw caution to the wind and produce a vaccine that he knows can be worse than the illness it’s supposed to protect against? Can it be the fact that vaccine manufacturers have no liability, whatsoever, for any damage or deaths their Covid-19 vaccines may cause?12 According to halacha (Shulchan Aruch, Yoreah Deah 155:1), one is not allowed to use a doctor whose reputation and pocketbook are not at stake. Since none of the vaccine manufacturers or doctors recommending and/or administering the vaccine have any responsibility for deaths or injuries that may occur so their reputations and income will not be affected, taking this vaccine is prohibited.
Ignored warnings
The following video13 was uploaded on March 27, 2020. In it, Drs. Hotez and Offit, noted vaccinologists, discuss the dangers of rushing a coronavirus vaccine because of ADE. Offit says that he does not expect a coronavirus vaccine to be ready for stage 3 efficacy trials within 2 years. Yet, only 9 months later, first Pfizer, and then Moderna, received Emergency Use Authorization from the FDA, to, basically, conduct the rest of their stage 3 trials on the entire world.14
Can ADE be avoided by repeat vaccinations?
The Israeli Prime Minister is betting on repeat vaccinations to avoid a potential disaster among the vaccinated (even as he’s still coercing everyone to vaccinate).
The People of Truth Association, in their appeal to the Israeli Supreme Court to stop human trials of the Pfizer Covid-19 vaccine, wrote that ADE was the reason that the Prime Minister has told those who vaccinated that they will need to keep vaccinating every six months.
The Prime Minister has announced in recent days in the media that due to the problem of lowering the level of antibodies after medical treatment, there is a real possibility that the recipients of the treatment will have to take the treatment every six months for their entire lives. This material fact was not revealed by the respondents to the recipients of the medical treatment before receiving it, but only now in retrospect, when the treatment cannot be stopped due to the phenomenon known as ADE, which endangers the lives of patients if they do not take the vaccine every six months.15
Conclusion
Emergency use authorization is normally given16 when, among other considerations, the FDA commissioner believes that:
-
… the known and potential benefits outweigh the known and potential risks of the product when used to diagnose, prevent, or treat the serious or life-threatening disease or condition that is the subject of the declaration; and
-
… there is no adequate, approved, and available alternative to the product for diagnosing, preventing, or treating such serious or life-threatening disease or condition.
The FDA, despite knowing that a coronavirus vaccine has a real risk of killing many more people over time than Covid-19,17 went ahead and authorized the vaccine for emergency use. One must ask why, especially since CDC data shows that most people are not even in danger of dying from Covid-19.18’19
The FDA has not approved any remedies for Covid-19, such as hydroxychloroquine,20’21 Ivermectin,22 and others,23 which are well-known and inexpensive drugs that been shown to successfully treat Covid-19 and which could have saved thousands of lives. Since the existence of any alternative remedies would have meant that a (highly lucrative24) vaccine could not be authorized, they have not approved these remedies.
Furthermore, this is the first time in history that billions of people, adults and children alike, are expected to be inoculated (with a goal of inoculating every person in the world).
Data gathered from multiple countries already shows that this vaccine is injuring and killing people in great numbers shortly after they get it.25 Yet, just like the risk of ADE was not enough to stop the development and authorization of these vaccines, so too are the growing numbers of injuries not enough to put a halt to this program.
Can there be a worse situation than the one we are facing? How can it be stopped?
Information about ADE in Hebrew: חיסון קורונה, תופעת ADE
Footnotes