Childhood Allergies
Childhood Allergies
Increase in Childhood Food Allergies
Photo courtesy of pixabay.com
If all children with food allergies in the United States were bused to school, they would fill up
103,704 (about 21%) of the 480,000 school buses on the road1.
Prevalence and dangers of food allergies in US children
Anaphylaxis is a serious and potentially fatal allergic reaction. It generally causes more than one of the following symptoms which occur within minutes or hours: an itchy rash, throat or tongue swelling, shortness of breath, vomiting, lightheadedness, and low blood pressure 2. Food allergies are known to cause life threatening anaphylactic reactions. Of the approximately 72,800,000 children under the age of 18 in the United States today, an estimated 5,600,000 (7%) have a food allergy. Of those, 2,240,000 (40%) are allergic to 2 or more foods. Anaphylactic reactions are experienced by over 40% of children who have food allergies. Children with known allergies often carry epi-pens containing epinephrine, a medication that can immediately stop an anaphylactic reaction. Statistics show that:
- Approximately 20-25 percent of epinephrine administrations in schools involve individuals whose allergy was unknown at the time of the reaction.
- Severe or fatal reactions can happen at any age, but teenagers and young adults with food allergies are at the highest risk of fatal food-induced anaphylaxis.
- Individuals with food allergies who also have asthma may be at increased risk for severe or fatal food allergy reactions.
- Most fatal food allergy reactions are triggered by food consumed outside the home.
- More than 15 percent of school-aged children with food allergies have had a reaction in school3.
An increasing problem
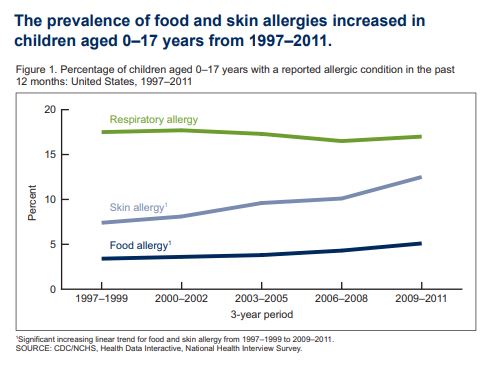
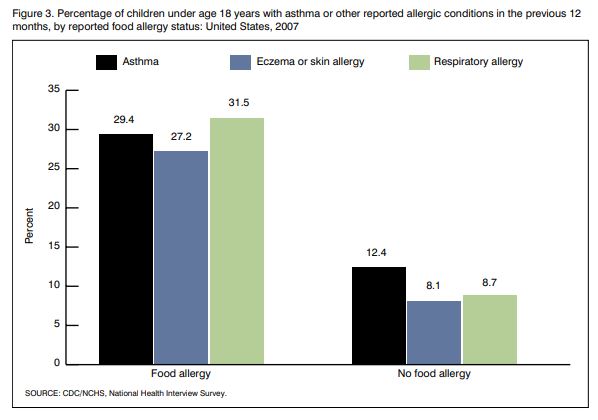
As the graphs below show, food and other allergies have been increasing over the past decades. Children with food allergies are more likely to have other allergies than children without food allergies.
Studies in individual states, such as this one in New York, show that anaphylactic allergic reactions represent the greatest number of hospitalizations.
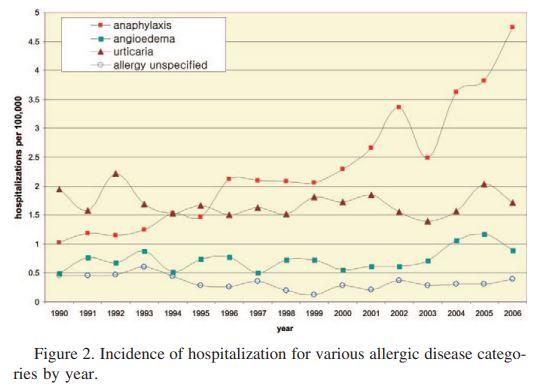
“The hospitalization rate for anaphylaxis was 1.0 per 100,000 in 1990 and increased to
4.7 per 100,000 by 2006. By 2002, the hospitalization rate for anaphylaxis exceeded the combined hospitalization rates for angioedema, urticaria, and allergy unspecified4.”
An international concern
Increasing rates of food allergies is a global problem as depicted by the graph below. Hospitalizations for children with food allergies have been increasing internationally, not just in the US.
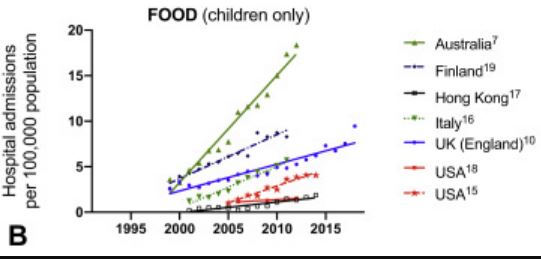
“In general, the increase in hospitalizations is predominantly due to
food-related anaphylaxis, particularly in children…5”
Food allergies were practically unknown as few as forty years ago.
“We’ve become so used to the prevalence of food allergies that it’s easy to forget that forty years ago, food allergies were nearly unheard of. The wave of serious allergies didn’t appear until the 80s, and a sudden spike in life-threatening food allergies began in the mid-1990s. In fact, food allergies increased by an astounding 377 percent between 2007 and 2017!”
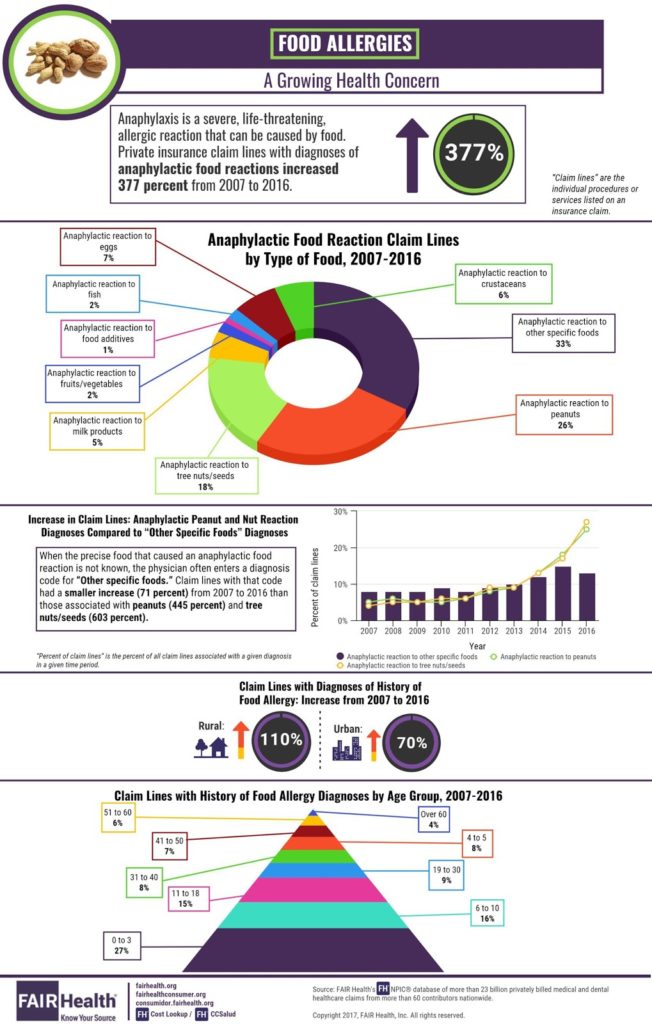
“The greatest rise in hospital reactions to eggs, wheat, and even gelatin are also on rise. On average, in every school classroom there are at least 2 children with life-threatening allergies and allergic reactions send 200,000 people to the hospital yearly.” admission for anaphylaxis has been due to peanut or tree nut allergies, but other food allergies are also becoming more common6.“
Related article:
Footnotes