The Fear Factor: Is It Justified?
Measles has become one of the most fear-laden words in public health.
When parents hear that measles is circulating, it is framed as something to be feared, and the conversation immediately jumps to vaccines. Rarely does anyone stop to explain what measles actually is, what a typical case looks like, or what the real risks are for a healthy, well-nourished child. But fear is not the same as information.
Before you can make a sound decision about vaccination, you need to understand the disease itself — what it does, who is genuinely at risk, how it was managed before the vaccine existed, and why the vaccine was developed in the first place. This article fills that gap.
What is measles?
Measles (rubeola) is a self-limiting, highly contagious respiratory virus that produces a rash all over the body. Incubation periods are usually between 14 and 21 days from the time of exposure.1
Symptoms include fever, runny nose, cough, rash, and eyes that become sensitive to light. White spots occur inside the mouth and progress to a rash that starts on the face and spreads to the rest of the body, which lasts for about a week. The rash can look similar to rashes symptomatic of other diseases, so it’s not easy for a doctor, much less a parent, to recognize.
The individual is contagious from about 4 days before to 4 days after the rash appears. Children who have had a naturally acquired measles infection usually develop long-lasting immunity.
Who actually gets seriously ill or dies?
Mortality
Measles is described by health agencies such as the CDC and the WHO as having a high mortality rate. However, the global figures, as the WHO also explains,2 are predominantly comprised of malnourished children from third-world countries with low per-capita income and/or weak health infrastructures. Natural disasters and wars serve to make a bad situation worse.
Complications are most common in children under 5 years and adults over age 30. They are more likely in children who are malnourished, especially those without enough vitamin A or with a weak immune system from HIV or other diseases.
…
Measles is still common, particularly in parts of Africa, the Middle East and Asia. The overwhelming majority of measles deaths occur in countries with low per capita incomes or weak health infrastructures that struggle to reach all children with immunization.
Damaged health infrastructure and health services in countries experiencing or recovering from a natural disaster or conflict interrupt routine immunization and overcrowding in residential camps increases the risk of infection. Children with malnutrition or other causes of a weak immune system are at highest risk of death from measles.
While the WHO only correlates poor health infrastructure with lack of immunization, malnourishment, vitamin A deficiency, and compromised immune systems from birth are independent risk factors that exist regardless of vaccination status and are likely reflections of poor health infrastructure, regardless of immunization concerns.
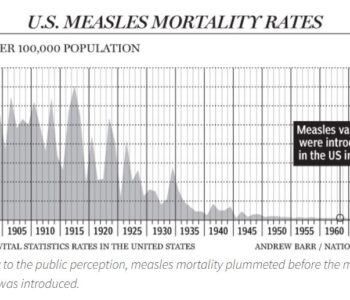
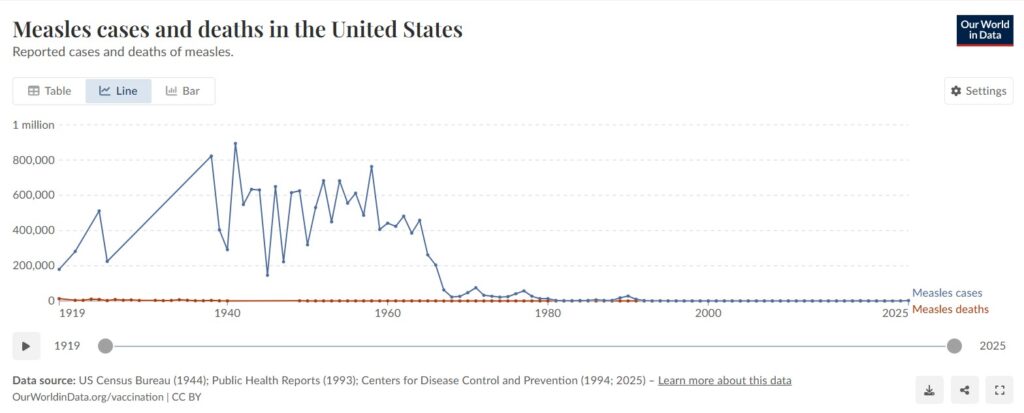
In the United States and other developed countries, the picture is totally different. While much fear-mongering is associated with measles infections, the death rate in the US has been virtually zero for decades. Here is a graph from Our World in Data from 1919-2025:3
What the CDC’s Own Data Reveals
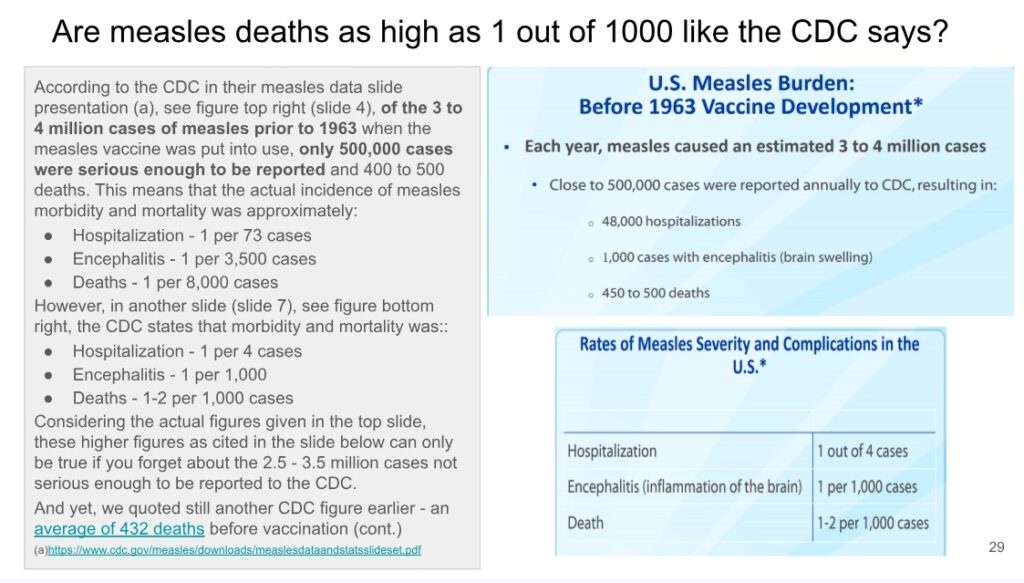
According to CDC data, in the five years before the vaccine was introduced there were an estimated 3-4 million cases annually, yet only 500,000 were serious enough to be reported. Based on the actual total case count, the real death rate was 1 in 8,000 — not the 1-2 per 1,000 the CDC cites, which is calculated only against reported cases and ignores the millions of mild, unreported ones.4
What about recent claims of death from measles?
In 2025, there have been claims of measles deaths in Texas and Israel.
Texas:
Regarding the Texas cases, The Defender, Children’s Health Defense News and Views site explained that doctors who looked at the children’s medical records released by the hospitals found that both deaths were attributable to pneumonia infections, which the hospitals did not treat properly.
Doctors who reviewed 8-year-old Daisy Hildebrand’s medical records disputed the Texas health authorities’ statement that she died from “measles pulmonary failure.” They said medical records show she died from acute respiratory distress “secondary to hospital-acquired pneumonia,” which she likely developed during a previous hospital stay.5
A child who died in a Texas hospital after developing pneumonia following a measles infection died as a result of “medical error” — including failure to administer the correct antibiotic in time, according to doctors who reviewed the child’s medical records, shared with Children’s Health Defense by the family. 6
Israel:
Regarding the children who were claimed to have died of measles in Israel, there are important unanswered questions about their care and why they deteriorated so severely.
From the media reports it appears that just about all the children who died passed away in a hospital.
- A doctor at Hadassah hospital, according to The Times of Israel 7 said most families waited too long before seeking help.
- The Health Ministry, according to Ynet News,8 reported on four children in intensive care at the same time, two of them on ECMO machines.
The public health response has focused entirely on vaccination and not at all on prevention/treatment or when to seek care. When a child reaches that point, the question isn’t just whether they got to the hospital in time, it’s what happened after they got there. Were they given vitamin A? Were they treated for the bacterial pneumonia that actually kills most measles patients? What did they really die from? None of this has been publicly addressed.
Morbidity
According to Physicians for Informed Consent (PIC):9
In the U.S. and other developed countries, 92% of hospitalized measles cases are low in vitamin A.
Research studies and national tracking of measles have documented the following:
- 1 in 10,000 or 0.01% of measles cases are fatal.
- 3 to 3.5 in 10,000 or 0.03-0.035% of measles cases result in seizure.
- 1 in 20,000 or 0.005% of measles cases result in measles encephalitis.
- 1 in 80,000 or 0.00125% of cases result in permanent disability from measles encephalitis.
- 7 in 1,000 or 0.7% of cases are hospitalized.
- 6 to 22 in 1,000,000 or 0.0006-0.0022% of cases result in subacute sclerosing panencephalitis (SSPE).
- 1 in 93,000 or 0.001% of measles cases with normal levels of vitamin A result in permanent disability or death.
Measles-associated immune amnesia
One of the adverse effects that has been attributed to the measles virus infection is immune amnesia, whereby the virus wipes out all previously acquired immunity, leaving the child susceptible to all illnesses afterwards. Tetyana Obukhanych explains that not only is this not a finding common to other illnesses, but a study done by Dr. Aaby found that children who were exposed to measles were less likely to die in the following 9 months to 4 years (depending on the study) than children who weren’t exposed.
In fact, they found that “exposed children developing clinical measles had lower age-adjusted mortality over the next 4 years than exposed children who did not develop clinical measles.”
…
“No long-term excess mortality after measles infection: a community study from Senegal” and “No persistent T lymphocyte immunosuppression or increased mortality after measles infection: a community study from Guinea-Bissau.”
…
Again, they found that “post-measles cases had significantly lower mortality than uninfected, non-immunized children in the following 9 months.”10
How was measles managed before the vaccine?
Doctors in the pre-vaccine era called measles an illness of mild to moderate severity and knew how to manage it:
Mild Ailment
…To date there have been close to 150 cases in the practice, and the numbers are now steadily decreasing. Like previous epidemics, the primary cases have been chiefly in the 5- and 6-year olds, with secondary cases in their younger siblings. No special features have been noted in this relatively mild epidemic. It has been mild because complications have occurred in only four children. One little girl aged 2 suffered from a lobular pneumonia, and three others developed acute otitis media following their measles. In the majority of children the whole episode has been well and truly over in a week, from the prodromal phase to the disappearance of the rash, and many mothers have remarked “how much good the attack has done their children,” as they seem so much better after the measles.
…
It is conspicuous that the 5-15 years age groups contained the vast majority of the cases. No effort was made to prevent the spread of the disease, except the ordinary precaution of not permitting juvenile visitors. Gamma globulin to thwart the onset of the disease was never used, since the few cases seen affecting the adults have always been severe. It is felt advisable to get the infection over in childhood and thus avoid this hazard later in life.”11
Dr. Suzanne Humphries, in her book Dissolving Illusions,12 co-authored with Roman Bystrianyk, explains how to treat measles by addressing underlying nutritional deficiencies.
Vitamin A stops the measles virus from rapidly multiplying inside cells by up-regulating the innate immune system in uninfected cells which helps to prevent the virus from infecting new cells. It is well known today that a low vitamin A level correlates with low measles-specific antibodies and increased morbidity and mortality. Vitamin A is a well-proven intervention for reduction of mortality, concomitant infections, and hospital stay.
It made no more sense to vaccinate against measles in 1963 than it does to put an infected child in a dark room instead of just giving vitamin A, which protects the retinas and the uninfected cells. In Africa, it’s the massive bodily demand for vitamin A that causes xeropthalmia (dry eyes) which, even long term, is reversible with vitamin A supplements.
The efficiency of the cellular immune system is tied to the intake of dietary nutrients, including vitamin A, vitamin C, zinc, selenium, and protein rich in vitamin B. Poor nutrition leads to impaired cellular immune responses, which results in worse outcomes after measles infection or exposure.
When the body fights any infection, especially measles, vitamin A stores become depleted by various mechanisms. Measles infections and high-titer measles vaccines both impair cell mediated immunity, in part because of vitamin A depletion. . . .
Because measles usually resolves on its own, only rest and hydration are generally necessary. When treatment is recommended, PIC suggests including the following:
- High-dose vitamin A
- Immune globulin (available for immunocompromised patients, such as those on chemotherapy)
- The antiviral medication, ribavirin
For more information about treating vaccinated and unvaccinated children for childhood diseases, read “The Unvaccinated Child: A Treatment Guide for Parents and Caregivers” by Eli Camp ND DHANP.13 From the book description:
The Unvaccinated Child is an unparalleled naturopathic treatment guide for common childhood illnesses. Its style is reader friendly for parents without a medical background or for practitioners looking for treatment options to offer their patients.
Why was the vaccine developed?
Dr. Langmuir, who was instrumental in developing the measles vaccine, had this to say about the disease and why he developed it:
… This self-limiting infection of short duration, moderate severity, and low fatality has maintained a remarkably stable biological balance over the centuries…
…
Thus, in the United States measles is a disease whose importance is not to be measured by total days disability or number of deaths, but rather by human values and by the fact that tools are becoming available which promise effective control and early eradication.
To those who ask me, “Why do you wish to eradicate measles?,” I reply with the same answer that Hillary used when asked why he wished to climb Mt. Everest. He said, “Because it is there.” To this may added, “…and it can be done.”14
What about natural immunity?
Immunization is constantly being suggested as an easy and sure way to get good immunity against measles. Is it better than natural immunity? Not according to Dr. Paul Offit, a noted pediatrician and vaccinologist who practices at Children’s Hospital of Philadelphia, and is often called on to treat children with measles.
The following clip from The Highwire shows Dr. Offit being interviewed by ZDogg (Dr. Zubin Damania). Dr. Offit had this to say about the superiority of natural immunity.15
ZDogg:
How comfortable are you with your own immunity and titers that hang around measles kids?
Offit:
I had measles.
ZDogg:
Oh, you had it.
Offit:
I’m of an age where I likely had it. I was born before 1957.
ZDogg:
So you cheated and had measles. So I’m just going to go on record and say Paul Offit says have a measles party everyone!
Offit:
Isn’t it true that after being naturally infected with measles I probably have higher frequencies of memory immune cells, B and T cells, than does someone who was vaccinated? Yes I do, that’s true.
ZDogg:
So you had a bigger antigen response.
Offit:
Yeah, the virus reproduced itself thousands of times in me and not the ten or twenty times it is when you get the vaccine. So I have a much greater immune response, it’s true.
Are there benefits to getting measles?
It has been found that children who contract measles are less likely to have allergies. It has also been found to be protective later in life, reducing the risk of heart attacks, strokes, and certain types of cancers.
For more on the documented benefits of natural measles infection, including its relationship to cancer research, see: Beneficial Effects of Childhood Infections.
Where to go from here?
Now that you have a clearer picture of what measles is and what it does, you are better equipped to evaluate what you are being told about the vaccine. The following posts will take you further:
- My Vaccine Journey
- Measles and the Measles Vaccine: What You Need to Know Before Consenting to Vaccinate Your Child
- Measles Vaccine: A Critical Lesson from the Ukraine
- Dr. Andrew Wakefield: Defended? Exonerated?
- Vaccine Policies: Can They Keep Your School or Shul Free of Disease Outbreaks?
Footnotes